First-time horse buyers are often unsure of what exactly they should be looking for when buying a horse. They may be unfamiliar with horse terminology and what, exactly, owning a horse entails. Even some experienced horse owners still need assistance when purchasing a new horse. If you are new to horses, always take an experienced horse person with you. They will know some things to look for. We’ve compiled a short list of things to consider when going to see a potential horse.
1. Does the horse have any past issues with colic, lameness, Cushings, etc? And have they had their vaccines/coggins? It is always important to try and get the vet records from any horse you are going to purchase. Some people say they vaccinated the horse themselves but have no proof. Rabies vaccines can only be purchased and given by a veterinarian. It is also good to ask if the horse is on anything for maintenance, such as supplements or joint injections.
2. Request a pre-purchase exam from a third-party veterinarian. Whatever you plan is for your horse, it is important to get a complete and thorough physical exam of the horse before you buy. X-rays of the legs and feet are often included in a pre-purchase exam, as well. It is equally important to have a vet that has a good reputation and is not connected to either the buyer or the seller perform the exam.
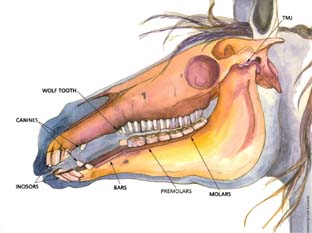
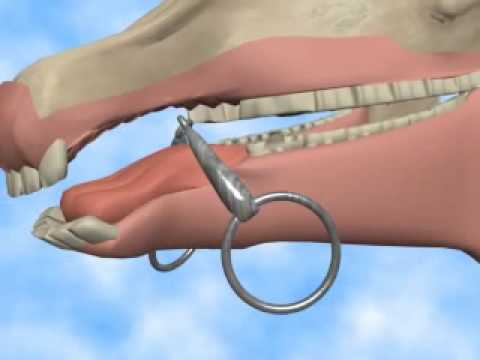
3. Have the horse aged by a veterinarian or certified equine dentist. We get clients all the time that ask us to come and confirm a horse’s age before they buy. We have had clients buy a horse, and then find out it is older/younger than what they seller told them once we check them out. One of the most extreme cases we have seen even had papers confirming that the horse was 5 years old. When we opened up his mouth, he was closer to 20 years old. Most sellers will say a horse is between 10-15 years old, even if they aren’t sure.
4. Ask to take the horse on trial for 7-10 days. This will allow you to see how the horse acts and rides outside its home environment. It will also enable you to see if the horse had been sedated when you tried it out on the farm. There are some shady people out there that will drug a horse to make it quieter when people come to try it out. Be sure to get a written agreement for the trial period!
5. Is the horse a good match for the capabilities of the rider? Some people buy a horse just because it’s pretty or flashy. They don’t consider the fact that the horse doesn’t have any training and they won’t be able to handle or ride it without sending it to a trainer. It is always important to consider your own skills and the training of the horse. For example, if you’re just learning how to ride, don’t buy a horse that is green broke and needs more training. Sure, that black horse with 4 white socks in the field my be pretty, but he’s also an unbroke 4-year-old stallion. Not something for an inexperienced or novice owner.
6. ALWAYS budget what it’s going to cost you to keep the horse. Buying the horse is often the least expensive part of horse ownership. You have to consider everything that goes into owning a horse long term. This includes: vet bills, farrier visits every 4-6 weeks, board costs, feed costs, tack, lessons, training, etc. Cheaper services are often not worth the cost of inferior work. A $3,000 horse can easily turn into an $8-10,000 horse by the end of a year. Insurance is a very good option for horse owners to consider. It can help cover the cost of expensive services and emergencies.
The take-home message from all of this is: be sure of what you are buying. All too often, people end up with buyer’s remorse because they didn’t check off all the boxes before signing the check. If you are ever unsure of a horse’s age, don’t hesitate to give us a call! Teeth are our specialty, after all!
Written by: Morgan Bosch, DVM
Advanced Equine Dentistry